Registered Nurse RN
Registered Nurse, Free Care Plans, Free NCLEX Review, Nurse Salary, and much more. Join the nursing revolution.

Protrusion, Retrusion, and Excursion Anatomy
In this anatomy lesson, I’m going to demonstrate protrusion, retrusion, and excursion , which are special body movement terms in anatomy that refer to forward (anterior), backward (posterior), or side to side movements.
Protrusion in Anatomy
Protrusion refers to the movement of a structure in an anterior (forward) direction. In fact, the word protrude means “projecting something forward.”
I call protrusion the kissing movement because it occurs when you pucker your lips like you’re going to give someone a kiss or stick out your tongue. Moving the mandible (lower jaw) forward is also an example of protrusion.

Retrusion in Anatomy
Retrusion is the opposite of protrusion. It refers to the movement of a structure in a posterior, or backward, direction. Putting your tongue back in your mouth, moving the lips back, or moving the mandible back are all examples of retrusion in anatomy.

Excursion in Anatomy
Finally, we have excursion , which refers to the side-to-side movement of the lower jaw (mandible). If you’ve ever heard of a character named Ernest P. Worrell, then you’ve definitely seen the excursion movement. He’s the character in those movies such as Ernest Goes to Camp, Ernest Goes to Jail, etc. When Ernest saw something nasty, he’d move his jaw back and forth and say, “Ewwww.”

Excursion can occur in either direction, and anatomists use directional terms to specify the type of excursion. When the mandible moves to either the left or right, it’s moving away from the body’s midline, so it’s called lateral excursion . When the mandible moves closer to the midline of the body, it’s called medial excursion .

Protrusion and Retrusion vs Protraction and Retraction
What about protraction and retraction ? Some anatomy textbooks will refer to the forward movement of the mandible, lips, or tongue as protraction (instead of protrusion), and the backward (posterior) movement will be called retraction (instead of retrusion). The terms are sometimes used interchangeably, so use whatever method your anatomy professor suggests (they give you the grade, not me!).
However, some anatomists today use protraction and retraction to refer almost exclusively to the scapulae, as it is a combined movement (protraction is anterolateral, and retraction is posteromedial). In contrast, protrusion and retrusion are more of an anterior/posterior movement. Then again, some anatomists prefer not to use protraction and retraction at all, even when describing shoulder blade movement.
Protrusion, Retrusion, and Excursion in Healthcare
Healthcare professionals use protrusion, retrusion, and excursion when documenting, performing assessments on patients, or treating disorders. For example, in her head-to-toe assessment , Nurse Sarah asked me to stick out my tongue (an example of protrusion), to assess cranial nerve twelve .
In addition, something called a mandibular protrusion test (MPT) is sometimes used by anesthesiologists to predict difficult airways in patients.
Free Quiz and More Anatomy Videos
Take a free protrusion vs retrusion quiz to test your knowledge, or review our protrusion vs retrusion video . In addition, you might want to watch our anatomy and physiology lectures on YouTube, or check our anatomy and physiology notes .
Please Share:
- Click to print (Opens in new window)
- Click to share on Facebook (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to share on Pinterest (Opens in new window)
- Click to share on Reddit (Opens in new window)
- Click to share on LinkedIn (Opens in new window)
- Click to share on WhatsApp (Opens in new window)
- Click to share on Pocket (Opens in new window)
- Click to share on Telegram (Opens in new window)
Disclosure and Privacy Policy
Important links, follow us on social media.
- Facebook Nursing
- Instagram Nursing
- TikTok Nurse
- Twitter Nursing
- YouTube Nursing
Copyright Notice

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
9.6: Types of Body Movements
- Last updated
- Save as PDF
- Page ID 68818

Learning Objectives
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table \(\PageIndex{1}\) ). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure \(\PageIndex{1}\) as you go through this section.
Interactive Link
Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?
Flexion and Extension
Flexion and extension are typically movements that take place within the sagittal plane and involve anterior or posterior movements of the neck, trunk, or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or trunk, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion of the vertebral column occurs in the coronal plane and is defined as the bending of the neck or trunk toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure \(\PageIndex{1}\) a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure \(\PageIndex{1}\) e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure \(\PageIndex{1}\) e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure \(\PageIndex{1}\) f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure \(\PageIndex{1}\) g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure \(\PageIndex{1}\) h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure \(\PageIndex{1}\) i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure \(\PageIndex{1}\) j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure \(\PageIndex{1}\) k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure \(\PageIndex{2}\) l).
9.5 Types of Body Movements
Learning objectives.
By the end of this section, you will be able to:
Define and identify the different body movements
- Demonstrate the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The degree and type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 9.1 ). Movement types are generally paired, with one directly opposing the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 9.5.1 as you go through this section.
External Website

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior motions are flexion and all posterior motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 9.5.1 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 9.5.1 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 9.5.1 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 9.5.1 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 9.5.2 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 9.5.2 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 9.5.2 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 9.5.2 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 9.5.2 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 9.5.2 l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
Review Questions
1. Briefly define the types of joint movements available at a ball-and-socket joint.
2. Discuss the joints involved and movements required for you to cross your arms together in front of your chest.
Answers for Critical Thinking Questions
- Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
- To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
This work, Anatomy & Physiology, is adapted from Anatomy & Physiology by OpenStax , licensed under CC BY . This edition, with revised content and artwork, is licensed under CC BY-SA except where otherwise noted.
Images, from Anatomy & Physiology by OpenStax , are licensed under CC BY except where otherwise noted.
Access the original for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction .
Anatomy & Physiology Copyright © 2019 by Lindsay M. Biga, Staci Bronson, Sierra Dawson, Amy Harwell, Robin Hopkins, Joel Kaufmann, Mike LeMaster, Philip Matern, Katie Morrison-Graham, Kristen Oja, Devon Quick, Jon Runyeon, OSU OERU, and OpenStax is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
9.5 Types of Body Movements
Learning objectives.
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 9.1 ). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 9.12 as you go through this section.
Interactive Link
Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?
Flexion and Extension
Flexion and extension are typically movements that take place within the sagittal plane and involve anterior or posterior movements of the neck, trunk, or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or trunk, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion of the vertebral column occurs in the coronal plane and is defined as the bending of the neck or trunk toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 9.12 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 9.12 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 9.12 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 9.12 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 9.13 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 9.13 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 9.13 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 9.13 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 9.13 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 9.13 l ).
As an Amazon Associate we earn from qualifying purchases.
This book may not be used in the training of large language models or otherwise be ingested into large language models or generative AI offerings without OpenStax's permission.
Want to cite, share, or modify this book? This book uses the Creative Commons Attribution License and you must attribute OpenStax.
Access for free at https://openstax.org/books/anatomy-and-physiology-2e/pages/1-introduction
- Authors: J. Gordon Betts, Kelly A. Young, James A. Wise, Eddie Johnson, Brandon Poe, Dean H. Kruse, Oksana Korol, Jody E. Johnson, Mark Womble, Peter DeSaix
- Publisher/website: OpenStax
- Book title: Anatomy and Physiology 2e
- Publication date: Apr 20, 2022
- Location: Houston, Texas
- Book URL: https://openstax.org/books/anatomy-and-physiology-2e/pages/1-introduction
- Section URL: https://openstax.org/books/anatomy-and-physiology-2e/pages/9-5-types-of-body-movements
© Dec 19, 2023 OpenStax. Textbook content produced by OpenStax is licensed under a Creative Commons Attribution License . The OpenStax name, OpenStax logo, OpenStax book covers, OpenStax CNX name, and OpenStax CNX logo are not subject to the Creative Commons license and may not be reproduced without the prior and express written consent of Rice University.
- Anatomical Position
- Body Planes
- Terms of Movement
- Terms of Location
- Embryology Terms
- Classification
- Synovial Joint
- Joint Stability
- Skeletal Muscle
- Blood Vessels
- Head and Neck
- Cardiovascular System
- Respiratory System
- Urinary System
- Reproductive System
- Central Nervous System
- Cranial Fossae
- Pterygopalatine Fossa
- Infratemporal Fossa
- Mastoid Fossa
- Frontal Bone
- Sphenoid Bone
- Ethmoid Bone
- Temporal Bone
- Occipital Bone
- Nasal Skeleton
- Cranial Foramina
- Facial Expression
- Extraocular
- Mastication
- Sympathetic Innervation
- Parasympathetic Innervation
- Ophthalmic Nerve
- Maxillary Nerve
- Mandibular Nerve
- Nose and Sinuses
- Salivary Glands
- Oral Cavity
- Arterial Supply
- Venous Drainage
- Lacrimal Gland
- Basal Ganglia
- Pineal Gland
- Pituitary Gland
- Spinal Cord (Grey Matter)
- Medulla Oblongata
- Ascending Tracts
- Descending Tracts
- Visual Pathway
- Auditory Pathway
- Olfactory Nerve (CN I)
- Optic Nerve (CN II)
- Oculomotor Nerve (CN III)
- Trochlear Nerve (CN IV)
- Trigeminal Nerve (CN V)
- Abducens Nerve (CN VI)
- Facial Nerve (CN VII)
- Vestibulocochlear Nerve (CN VIII)
- Glossopharyngeal Nerve (CN IX)
- Vagus Nerve (CN X)
- Accessory Nerve (CN XI)
- Hypoglossal Nerve (CN XII)
- Dural Venous Sinuses
- Cavernous Sinus
- Anterior Triangle
- Posterior Triangle
- Cervical Spine
- Thyroid Gland
- Parathyroid Glands
- Suboccipital
- Suprahyoids
- Infrahyoids
- Phrenic Nerve
- Cervical Plexus
- Fascial Layers
- Tonsils (Waldeyer's Ring)
- Superior Mediastinum
- Anterior Mediastinum
- Middle Mediastinum
- Posterior Mediastinum
- Thoracic Spine
- Thoracic Cage
- Thymus Gland
- Mammary Glands
- Tracheobronchial Tree
- Superior Vena Cava
- Vertebral Column
- Superficial
- Intermediate
- Spinal Cord
- Quadrangular Space
- Triangular Interval
- Triangular Space
- Cubital Fossa
- Ulnar Tunnel
- Extensor Compartments
- Ulnar Canal
- Carpal Tunnel
- Anatomical Snuffbox
- Pectoral Region
- Shoulder Region
- Anterior Forearm
- Posterior Forearm
- Brachial Plexus
- Axillary Nerve
- Musculocutaneous Nerve
- Median Nerve
- Radial Nerve
- Ulnar Nerve
- Acromioclavicular Joint
- Sternoclavicular Joint
- Shoulder Joint
- Elbow Joint
- Radioulnar Joints
- Wrist Joint
- Metacarpophalangeal Joint
- Proximal Interphalangeal Joint
- Extensor Tendon Expansion
- Flexor Pulley System
- Femoral Triangle
- Femoral Canal
- Adductor Canal
- Popliteal Fossa
- Tarsal Tunnel
- Fascia Lata
- Gluteal Region
- Cutaneous Innervation
- Lumbar Plexus
- Sacral Plexus
- Femoral Nerve
- Obturator Nerve
- Sciatic Nerve
- Tibial Nerve
- Common Fibular Nerve
- Superficial Fibular Nerve
- Deep Fibular Nerve
- Tibiofibular Joints
- Ankle Joint
- Subtalar Joint
- Foot Arches
- Walking and Gaits
- Abdominal Cavity
- Calot’s Triangle
- The Peritoneum
- Inguinal Canal
- Hesselbach's Triangle
- Lumbar Spine
- Anterolateral Abdominal Wall
- Posterior Abdominal Wall
- Small Intestine
- Gallbladder
- Adrenal Glands
- Sciatic Foramina
- Pelvic Girdle
- Sacroiliac Joint
- Pelvic Floor
- Urinary Bladder
- Testes and Epididymis
- Spermatic Cord
- Prostate Gland
- Bulbourethral Glands
- Seminal Vesicles
- Fallopian (Uterine) Tubes
- Supporting Ligaments
- Pudendal Nerve
- Female Body
- Female Pelvis
- Male Pelvis
- Cardiovascular
- Gastrointestinal
- Respiratory
- Female Reproductive
- Male Reproductive
Anatomical Terms of Movement
Original Author(s): Oliver Jones Last updated: May 30, 2020 Revisions: 27
- 1 Flexion and Extension
- 2 Abduction and Adduction
- 3 Medial and Lateral Rotation
- 4 Elevation and Depression
- 5 Pronation and Supination
- 6 Dorsiflexion and Plantarflexion
- 7 Inversion and Eversion
- 8 Opposition and Reposition
- 9 Circumduction
- 10 Protraction and Retraction
Anatomical terms of movement are used to describe the actions of muscles upon the skeleton. Muscles contract to produce movement at joints, and the subsequent movements can be precisely described using this terminology.
The terms used assume that the body begins in the anatomical position . Most movements have an opposite movement – also known as an antagonistic movement. We have described the terms in antagonistic pairs for ease of understanding.
Flexion and Extension
Flexion and extension are movements that occur in the sagittal plane. They refer to increasing and decreasing the angle between two body parts:
Flexion refers to a movement that decreases the angle between two body parts. Flexion at the elbow is decreasing the angle between the ulna and the humerus. When the knee flexes, the ankle moves closer to the buttock, and the angle between the femur and tibia gets smaller.
Extension refers to a movement that increases the angle between two body parts. Extension at the elbow is increasing the angle between the ulna and the humerus. Extension of the knee straightens the lower limb.
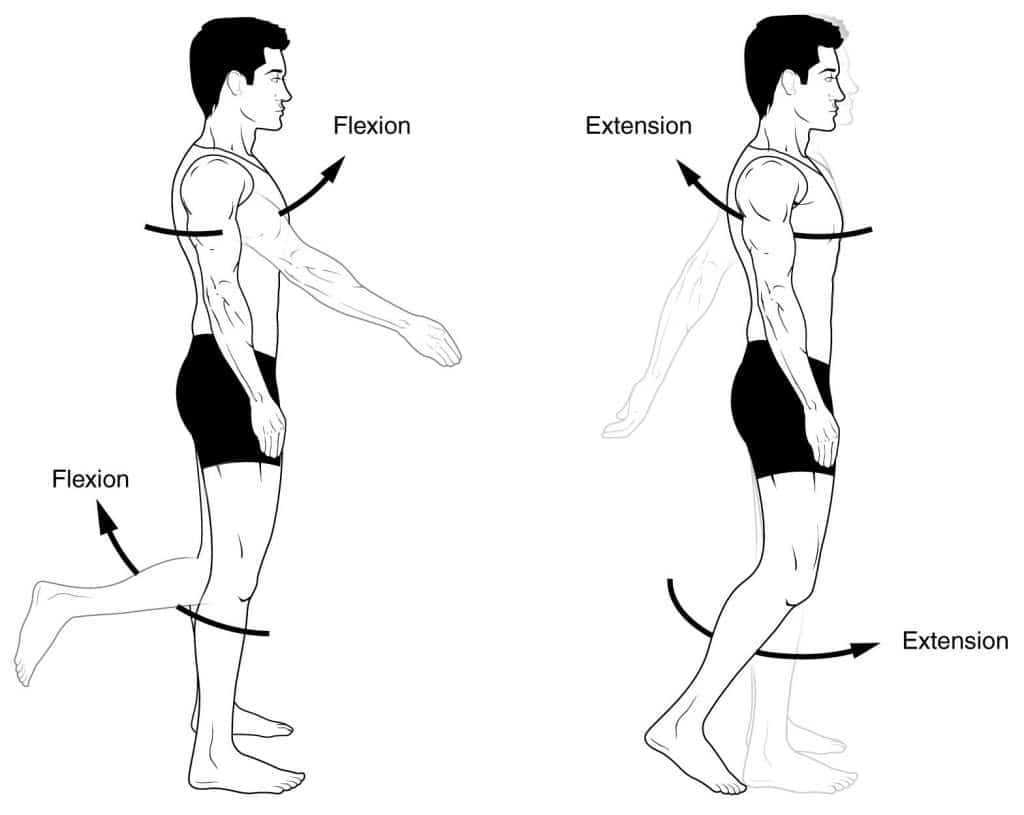
Fig 1 – Flexion and extension.
Abduction and Adduction
Abduction and adduction are two terms that are used to describe movements towards or away from the midline of the body.
Abduction is a movement away from the midline – just as abducting someone is to take them away. For example, abduction of the shoulder raises the arms out to the sides of the body.
Adduction is a movement towards the midline. Adduction of the hip squeezes the legs together.
In fingers and toes, the midline used is not the midline of the body, but of the hand and foot respectively. Therefore, abducting the fingers spreads them out.
Medial and Lateral Rotation
Medial and lateral rotation describe movement of the limbs around their long axis:
Medial rotation is a rotational movement towards the midline. It is sometimes referred to as internal rotation. To understand this, we have two scenarios to imagine. Firstly, with a straight leg, rotate it to point the toes inward. This is medial rotation of the hip. Secondly, imagine you are carrying a tea tray in front of you, with elbow at 90 degrees. Now rotate the arm, bringing your hand towards your opposite hip (elbow still at 90 degrees). This is internal rotation of the shoulder.
Lateral rotation is a rotating movement away from the midline. This is in the opposite direction to the movements described above.
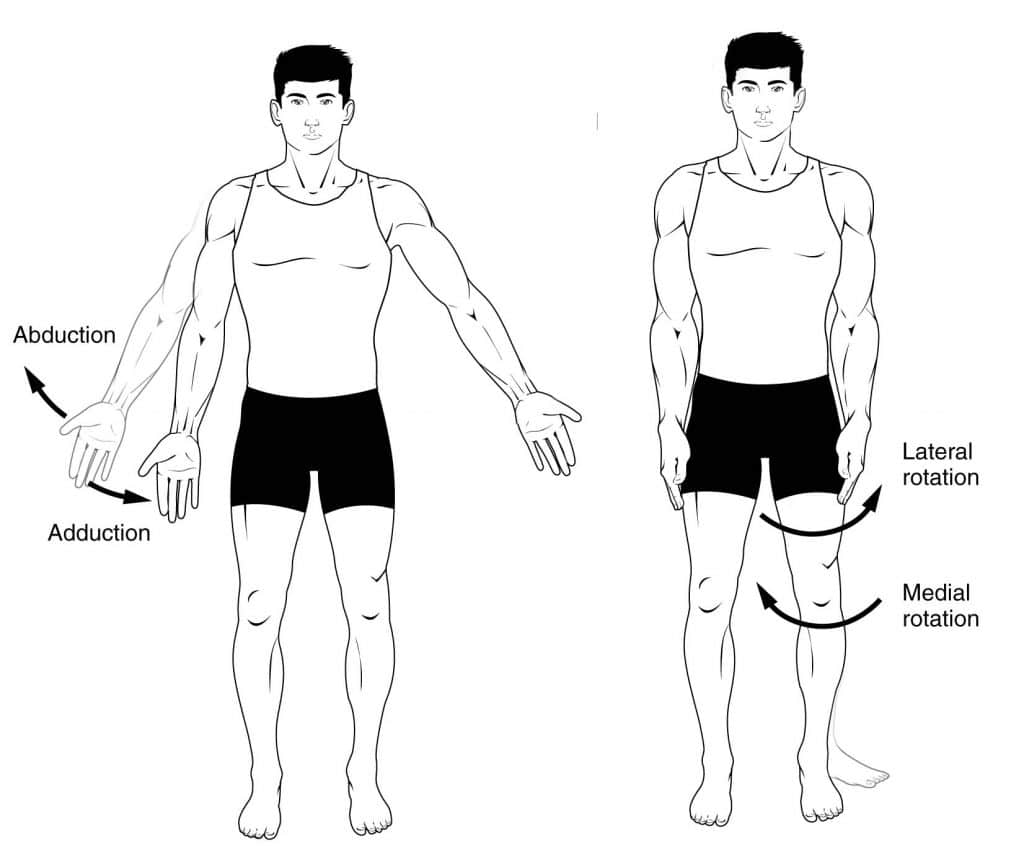
Fig 2 – Adduction, abduction and rotation.
Elevation and Depression
Elevation refers to movement in a superior direction (e.g. shoulder shrug), depression refers to movement in an inferior direction.
Pronation and Supination
This is easily confused with medial and lateral rotation, but the difference is subtle. With your hand resting on a table in front of you, and keeping your shoulder and elbow still, turn your hand onto its back, palm up. This is the supine position, and so this movement is supination .
Again, keeping the elbow and shoulder still, flip your hand onto its front, palm down. This is the prone position, and so this movement is named pronation .
These terms also apply to the whole body – when lying flat on the back, the body is supine. When lying flat on the front, the body is prone.
Dorsiflexion and Plantarflexion
Dorsiflexion and plantarflexion are terms used to describe movements at the ankle. They refer to the two surfaces of the foot; the dorsum (superior surface) and the plantar surface (the sole).
Dorsiflexion refers to flexion at the ankle, so that the foot points more superiorly. Dorsiflexion of the hand is a confusing term, and so is rarely used. The dorsum of the hand is the posterior surface, and so movement in that direction is extension . Therefore we can say that dorsiflexion of the wrist is the same as extension.
Plantarflexion refers extension at the ankle, so that the foot points inferiorly. Similarly there is a term for the hand, which is palmarflexion.
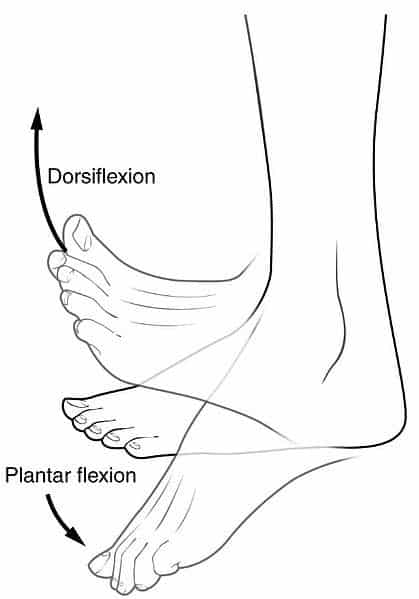
Fig 3 – Dorsiflexion and plantar flexion
Inversion and Eversion
Inversion and eversion are movements which occur at the ankle joint, referring to the rotation of the foot around its long axis.
Inversion involves the movement of the sole towards the median plane – so that the sole faces in a medial direction.
Eversion involves the movement of the sole away from the median plane – so that the sole faces in a lateral direction.
Opposition and Reposition
A pair of movements that are limited to humans and some great apes, these terms apply to the additional movements that the hand and thumb can perform in these species.
Opposition brings the thumb and little finger together.
Reposition is a movement that moves the thumb and the little finger away from each other, effectively reversing opposition.
Circumduction
Circumduction can be defined as a conical movement of a limb extending from the joint at which the movement is controlled.
It is sometimes talked about as a circular motion, but is more accurately conical due to the ‘cone’ formed by the moving limb.
Protraction and Retraction
Protraction describes the anterolateral movement of the scapula on the thoracic wall that allows the shoulder to move anteriorly. In practice, this is the movement of ‘reaching out’ to something.
Retraction refers to the posteromedial movement of the scapula on the thoracic wall, which causes the shoulder region to move posteriorly i.e. picking something up.
The terms used assume that the body begins in the anatomical position . Most movements have an opposite movement - also known as an antagonistic movement. We have described the terms in antagonistic pairs for ease of understanding.
Abduction is a movement away from the midline - just as abducting someone is to take them away. For example, abduction of the shoulder raises the arms out to the sides of the body.
These terms also apply to the whole body - when lying flat on the back, the body is supine. When lying flat on the front, the body is prone.
Inversion involves the movement of the sole towards the median plane - so that the sole faces in a medial direction.
Eversion involves the movement of the sole away from the median plane - so that the sole faces in a lateral direction.
It is sometimes talked about as a circular motion, but is more accurately conical due to the 'cone' formed by the moving limb.
Protraction describes the anterolateral movement of the scapula on the thoracic wall that allows the shoulder to move anteriorly. In practice, this is the movement of 'reaching out' to something.
Found an error? Is our article missing some key information? Make the changes yourself here!
Once you've finished editing, click 'Submit for Review', and your changes will be reviewed by our team before publishing on the site.
We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy .
Privacy Overview
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
11.10 Types of Body Movements
Learning Objectives
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint result from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 11.10.1). Movement types are paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 11.10.1 as you go through this section.

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 11.10.1a-d).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 11.10.1e).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 11.10.1e).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation. Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 11.10.1f). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 11.10.2g).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 11.10.2h).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilise the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 11.10.2i).
Protraction and Reaction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 11.10.2j.)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 11.10.2k).
Excursion is the side-to-side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a particularly important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 11.10.2l).
Table 11.10.1. Movements of the Joints
Section Review
The variety of movements provided by the several types of synovial joints allows for a broad range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate, and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
Fundamentals of Anatomy and Physiology Copyright © 2021 by University of Southern Queensland is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
- TheFreeDictionary
- Word / Article
- Starts with
- Free toolbar & extensions
- Word of the Day
- Free content
ex·cur·sion
- active assistive range of motion
- Acute Alcohol Intoxication
- aortocoronary bypass
- balancing side condyle
- Bennett movement
- Bilirubin and Bilirubin Fractions
- brain wave cycle
- breathing pattern, ineffective
- breathing-related sleep disorder
- clasp-knife rigidity
- clasp-knife spasticity
- Coagulation Factors
- concomitance
- coronary artery bypass
- exclusive provider organization
- exclusivity
- exclusivity period
- exconjugant
- excoriation
- excrementitious
- excrescence
- excrescency
- excretion urography
- excretory duct
- excretory duct of seminal gland
- excretory ducts of lacrimal gland
- excretory ductule of lacrimal gland
- excretory gland
- excretory organ
- excretory urography
- exculpatory
- excurvation
- excuse of infancy
- excycloduction
- excyclophoria
- excyclotropia
- excyclovergence
- excystation
- execution wound
- executive committee
- executive function
- executive information system
- executive letter
- Executive Monkey
- executive profile
- exemplar site
- exempt research
- exenatide acetate
- exencephalia
- exencephalic
- exculpating
- exculpation
- exculpations
- exculpatorily
- exculpatory clause
- Exculpatory evidence
- Excuria Recovery Services, LLC
- Excursion Inlet Seaplane Base
- Excursion Limit
- Excursion liner
- Excursion Maximum
- Excursion of Suspension
- excursion rate
- excursion steamer
- excursion ticket
- Excursion train
- Excursion trains
- excursionise
- excursionism
- excursionist
- excursionists
- excursionize
- Excursions Maritimes Tropéziennes
- excursively
- excursiveness
- Facebook Share

- school Campus Bookshelves
- menu_book Bookshelves
- perm_media Learning Objects
- login Login
- how_to_reg Request Instructor Account
- hub Instructor Commons
- Download Page (PDF)
- Download Full Book (PDF)
- Periodic Table
- Physics Constants
- Scientific Calculator
- Reference & Cite
- Tools expand_more
- Readability
selected template will load here
This action is not available.
12.6: Types of Body Movements
- Last updated
- Save as PDF
- Page ID 34490
Learning Objectives
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 1). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward.
Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

A YouTube element has been excluded from this version of the text. You can view it online here: pb.libretexts.org/aapi/?p=248
Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 1).

Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction, Adduction, and Circumduction

Abduction and adduction are motions of the limbs, hand, fingers, or toes in the coronal (medial–lateral) plane of movement. Moving the limb or hand laterally away from the body, or spreading the fingers or toes, is abduction. Adduction brings the limb or hand toward or across the midline of the body, or brings the fingers or toes together. Circumduction is the movement of the limb, hand, or fingers in a circular pattern, using the sequential combination of flexion, adduction, extension, and abduction motions.
Adduction, abduction, and circumduction take place at the shoulder, hip, wrist, metacarpophalangeal, and metatarsophalangeal joints.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 2).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 2).

Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 3). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Turning of the head side to side or twisting of the body is rotation. Medial and lateral rotation of the upper limb at the shoulder or lower limb at the hip involves turning the anterior surface of the limb toward the midline of the body (medial or internal rotation) or away from the midline (lateral or external rotation).
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 4).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 4).

Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 5).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 5.)

Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 6).

Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 6).
Contributors and Attributions
- Anatomy & Physiology. Authored by : OpenStax College. Provided by : Rice University. Located at : cnx.org/contents/[email protected] . License : CC BY: Attribution . License Terms : Download for free at cnx.org/contents/[email protected]

Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
Types of Body Movements
OpenStaxCollege
Learning Objectives
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( [link] ). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to [link] as you go through this section.

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?
.jpg#fixme "what is excursion in anatomy")
Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see [link] a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see [link] e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see [link] e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see [link] f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see [link] g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see [link] h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see [link] i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See [link] j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see [link] k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see [link] l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
The joints between the articular processes of adjacent vertebrae can contribute to which movement?
- lateral flexion
- circumduction
- dorsiflexion
Which motion moves the bottom of the foot away from the midline of the body?
- plantar flexion
Movement of a body region in a circular movement at a condyloid joint is what type of motion?
Supination is the motion that moves the ________.
- hand from the palm backward position to the palm forward position
- foot so that the bottom of the foot faces the midline of the body
- hand from the palm forward position to the palm backward position
- scapula in an upward direction
Movement at the shoulder joint that moves the upper limb laterally away from the body is called ________.
- lateral rotation
Critical Thinking Questions
Briefly define the types of joint movements available at a ball-and-socket joint.
Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
Discuss the joints involved and movements required for you to cross your arms together in front of your chest.
To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
Types of Body Movements Copyright © 2013 by OpenStaxCollege is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Multidiscip Respir Med
- v.17; 2022 Jan 12
Diaphragmatic excursion by ultrasound: reference values for the normal population; a cross-sectional study in Egypt
Ahmed e. kabil.
1 Chest Diseases Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt
2 Chest Diseases Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt
3 College of Medical Rehabilitation Sciences, Taibah University, Medina, Saudi Arabia
Mahmoud Elsaeed
Houssam eldin hassanin, ibrahim h. yousef, heba h. eltrawy, ahmed m. ewis, ahmed aboseif, abdallah m. albalsha, sawsan elsawy, abdul rahman h. ali.
4 Mahatma Gandhi University, Meghalaya, India
Publisher's note: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Measurement of diaphragmatic motion by ultrasound is being utilized in different aspects of clinical practice. Defining reference values of the diaphragmatic excursion is important to identify those with diaphragmatic motion abnormalities. This study aimed to define the normal range of diaphragmatic motion (reference values) by Mmode ultrasound for the normal population.
Healthy volunteers were included in this study. Those with comorbidities, skeletal deformity, acute or chronic respiratory illness were excluded. Diaphragmatic ultrasound in the supine position was performed using a lowfrequency probe. The B-mode was applied for diaphragmatic identification, and the M-mode was employed for the recording of the amplitude of diaphragm contraction during quiet breathing, deep breathing and sniffing.
The study included 757 healthy subjects [478 men (63.14%) and 279 women (36.86%)] with normal spirometry and negative history of previous or current respiratory illness. Their mean age and BMI were 45.17 ±14.84 years and 29.36±19.68 (kg/m 2 ). The mean right hemidiaphragmatic excursion was 2.32±0.54, 5.54±1.26 and 2.90±0.63 for quiet breathing, deep breathing and sniffing, respectively, while the left hemidiaphragmatic excursion was 2.35±0.54, 5.30±1.21 and 2.97±0.56 cm for quiet breathing, deep breathing and sniffing, respectively. There was a statistically significant difference between right and left diaphragmatic excursion among all studied subjects. The ratio of right to left diaphragmatic excursion during quiet breathing was (1.009±0.19); maximum 181% and minimum 28%. Only 19 cases showed a right to left ratio of less than 50% (5 men and 14 women). The diaphragmatic excursion was higher in males than females. There was a significant difference in diaphragmatic excursion among age groups. Age, sex and BMI significantly affected the diaphragmatic motion.
Conclusions
Diaphragmatic excursion values presented in this study can be used as reference values to detect diaphragmatic dysfunction in clinical practice. Diaphragmatic motion is affected by several factors including age, sex and body mass index.
Introduction
The diaphragm is the main muscle of respiration [ 1 ]. Diaphragmatic excursion is 1-2 cm during tidal breathing and 7-11 cm during deep inspiration [ 2 ]. The assessment of diaphragmatic function is important for diagnosis and follow up of various physiologic and pathologic conditions [ 1-4 ]. Several methods exist for the evaluation of diaphragmatic function. These methods include fluoroscopy [ 3 ], computed tomography [ 4 ], magnetic resonance imaging [ 2 ], and ultrasonography [ 5 ]. Thoracic ultrasound has been reported to be a useful tool for the examination of diaphragmatic function [ 6 ]. It is a bedside non-invasive tool that provides various techniques for evaluation of diaphragmatic function including measurement of diaphragmatic excursion and thickness as well as changes during different phases of inspiration [ 7 ]. Ultrasonography has been proved to be superior to fluoroscopy and can provide accurate measurement of diaphragmatic excursion [ 3 ]. Previous studies highlighted the lack of reference values for diaphragmatic excursion in the normal population which complicates diagnosing abnormal diaphragmatic motion in certain diseases. No data is available about diaphragmatic motion in the normal Egyptian population and no reference data are available to compare with. This study aimed to explore the normal diaphragmatic excursion in the Egyptian population by M-mode ultrasonography.
This is a cross-sectional study that initially included 780 participants. Twenty-three subjects were excluded due to poor images or failed visualization of one hemidiaphragm, rendering the finally included number 757 individuals (478 males and 279 females), all had normal lung functions with no history of chest disease. Smokers, those with acute respiratory illness, chronic respiratory disease, associated comorbidities, physical disability, abnormal pulmonary function tests or history of anesthesia within the past six months were excluded from the study.
Pulmonary functions were done using spirometry (Spirosift 5000; Fukuda Denshi, Beijing, China). The operator encouraged all subjects verbally to exhale as fast and as deep as possible. Each subject performed at least three technically accepted measurements, and the best of them was selected for statistical analysis. All measurements were performed according to ERS/ATS standards [ 7 ].
Diaphragmatic ultrasound
All sonographic examinations were done by the research team. Inter-operator and intra-operator variability were excellent (data not shown). Examinations were performed at quiet temperature (22-25C°). All subjects were asked to rest for 30 min before sonography. Ultrasonography was done using an ultrasound device (SSI6000; Sonoscape, Nanshan, China), while subjects located in the supine position. Examinations were performed using 3.5 MHz curvilinear probe. Each hemidiaphragm was first visualized by Bmode, then M-mode was used to evaluate diaphragmatic excursion in tidal breathing, deep breathing and sniff. The right hemidiaphragm was measured by positioning the probe between the midclavicular and midaxillary lines below the right costal margin (subcostal approach), using the liver as an acoustic window. The probe was directed medially, cephalic and dorsally. When the hemidiaphragm was well visualized, the M-mode was applied to measure the excursion [ 8 ]. The left hemidiaphragm was visualized using the spleen as an acoustic window. The probe was positioned between the left midclavicular and midaxillary lines below the left costal margin. The probe was directed in the same way as the right side [ 8 ]. Targeting to improve visualization of the left hemidiaphragm, and overcome the small acoustic window of spleen, the probe was sometimes displaced caudally in the abdomen to obtain a better angle for visualization. The diaphragm was seen as a single echogenic line ( Figure 1 ), moving towards the probe during inspiration and away from the probe during expiration [ 5 ]. Diaphragmatic excursion was defined as the difference between the highest point and steep point (amplitude). The diaphragmatic excursion was recorded in different respiratory phases; tidal breathing (normal quiet inspiration), deep inspiration (holding up breathing after maximal inspiration), and sniffing (quick nasal inspiration with a closed mouth) ( Figure 2 ). The direction of movement was also observed (normal or paradoxical), as absent or paradoxical motion may indicate diaphragm paralysis.
Statistical analysis
All data were analyzed by SPSS (Statistical Package for Social Sciences) software version 19 (IBM corp., Armonk, NY, USA) after data cleaning and check. Numerical data were presented as mean ±SD, while categorical data were presented as number (percentage). Independent sample t-test and ANOVA were used for comparisons, Pearson correlation coefficient for testing the relationship between diaphragmatic excursion and demographic parameters, and linear regression analysis for the detection of factors affecting diaphragmatic motion. The significance level was set at a p≤0.05.
Totally, 757 healthy subjects with normal spirometry were included in this study [478 men (63.14%) and 279 women (36.86%)]. The mean age of the study population was 45.17±14.84 years. Men were significantly older, had significantly higher FVC% and VT%, while women had significantly higher body mass index (BMI) and better FEF25-75% ( Table 1 ). There was a statistically significant difference between right and left diaphragmatic excursion among all studied subjects ( Table 2 ). The ratio of right to left diaphragmatic excursion during quiet breathing was (1.009±0.19); maximum 181% and minimum 28%. Only 19 cases showed a right to left ratio less than 50% (5 men and 14 women). Right diaphrag- matic motion was significantly higher in men than in women ( Table 3 ). There were significant differences in diaphragmatic excursion among age groups ( Table 4 ). However, there were no statistically significant differences among BMI categories ( Table 5 ). A statistically significant positive correlation was found between age and right diaphragmatic excursion during both deep breathing and sniffing, and between age and left hemidiaphragmatic excursion during deep breathing (r=0.045, p˂0.001, r=0.117, p=0.001, r=0.190, p˂0.001, respectively). A statistically significant negative correlation was observed between age and left hemidiaphragmatic excursion during quiet breathing (r=-0.098, p=0.007). On the other hand, a statistically significant negative correlation was detected between BMI and right hemidiaphragmatic excursion during deep breathing and sniffing, and between BMI and left hemidiaphragmatic excursion during deep breathing (r = 0.182, p˂0.001; r = -0.094, p=0.009; r = -0.142, p˂0.001, respectively). A positive correlation between BMI and left hemidiaphragmatic excursion was found during quiet breathing (r = 0.148, p˂0.001) ( Table 6 ). Regression analysis revealed that sex, age, BMI and pulmonary functions affect diaphragmatic motion (good predictors). Age, sex and BMI index significantly affect diaphragmatic motion by variable extents during different types of breathing.

Right diaphragm visualization by B-mode ultrasound. The diaphragm is seen as a thick white line moving with respiration. The liver is used as an echogenic window.

Visualization and measurement of right diaphragmatic excursion by M-mode ultrasound. The diaphragm is seen as a white line moving with respiration. The diaphragmatic excursion is measured as the amplitude of wave seen in M-mode during breathing.
Demographic data and pulmonary functions of the studied population.
# Comparison between men and women
* p<0.05.
Diaphragmatic excursion in the normal population.
Diaphragmatic excursion according to sex.
# Comparison between men and women; *p<0.05.
Diaphragm accounts for three fourths of lung ventilation [ 9 ]. Diaphragmatic imaging is important for the diagnosis of diaphragmatic dysfunction or paralysis [ 3 , 9 ]. Normal values of diaphragmatic excursion are important to evaluate abnormalities in different diseases [ 8 ]. Diaphragmatic dysfunction (weakness or paralysis) is usually underdiagnosed in clinical practice [ 10 ]. Normal values can be used to detect either hypokinesia or hyperkinesia [ 11 ]. In this study we found that the mean diaphragmatic excursion for right hemidiaphragm during quiet breathing was 2.32±0.54 cm, while that for the left one was 2.35±0.54 cm. The mean diaphragmatic excursion during deep breathing was 5.54±1.26 cm for the right side and 5.30±1.21 cm for the left, whereas the excursion during sniffing was 2.90±0.63 cm for the right side and 2.97±0.56 cm for the contralateral hemidiaphragm. These results are in line with the results of previous reports [ 5-7 ]. Normal diaphragmatic excursion in tidal breathing in previous studies was reported to be from 1-2.5 cm [ 8 ]. These values can be affected by age, sex, body composition [ 12 , 13 ], scanning position, and phase of inspiration [ 14 ]. Right diaphragmatic excursion was shown to be significantly better in men than in women ( Table 3 ). The same results were reported by Kantarci et al . who in their study reported a significant difference in diaphragmatic motion between male and female subjects [ 13 ]. In their study, sex was the most significant factor affecting diaphragmatic function. In our study, there was a significant difference in diaphragmatic excursion among age groups ( Table 4 ). Similar results were reported in previous studies [ 6 , 8 ]. Boussuges et al. [ 8 ] reported a higher diaphragmatic excursion in men than women in all types of breathing. This can be attributed to differences in height, weight, age [ 6 , 8 ], diaphragmatic mass, diaphragmatic fiber type property, metabolic activity, contractile properties and environmental factors [ 9 ].
In the current study, a statistically significant positive correlation was observed between age and diaphragmatic excursion during both deep breathing and sniffing in the right side, and during deep breathing only in the left one. Besides, a statistically significant negative correlation was revealed between age and left hemidiaphragmatic excursion during quiet breathing ( Table 4 ). Kantarci et al . [ 13 ] found that diaphragmatic function is significantly lower in the individuals below 30 years when compared to those aged more than 30 years.
We did not find any significant statistical differences among BMI categories ( Table 5 ). However, there was a significant positive correlation between BMI and left hemidiaphragmatic excursion during quiet breathing ( Table 6 ). Moreover, regression analysis showed that age, sex and BMI are the main factors that significantly affect diaphragmatic excursion. Kantarci et al . [ 13 ] reported a significant difference in diaphragmatic motion according to BMI categories and explained this by the difference in fat and muscle composition. In the same context, Scarlata et al . [ 12 ] reported a significant correlation between diaphragmatic motion and gender, age, weight and height. This difference is clinically important for the identification of those with a risk of low diaphragmatic function to include them in rehabilitation programs. This discrepancy between studies may be due to different demographic characters and distribution of population in different body mass index categories. Increased diaphragmatic motion with increased BMI may be attributed to differences in height or the increased diaphragm weight with increased body weight [ 10 ]. This can be confirmed through the assessment of diaphragmatic thickness by ultrasonography.
Diaphragmatic excursion according to age groups.
Diaphragmatic excursion according to BMI.
Correlation with body mass index and age and diaphragmatic excursion.
BMI, body mass index; **correlation is significant at the 0.01 level (2-tailed).
The strengths of this study include the large number of studied populations, different age groups and body composition. This study reflects the normal distribution of diaphragmatic excursion in the normal population in Egypt. Knowing normal references for diaphragmatic ultrasound measurements can be of clinical value in identifying and diagnosing diaphragmatic paralysis, as well as exploring the cause and predicting the prognosis of diaphragm paralysis [ 15 ]. Diaphragmatic ultrasound normal values can be also used to predict the response to treatment as in rehabilitation programs, in addition to setting cut-off values to predict successful weaning parameters from mechanical ventilation. Likewise, it can be used to evaluate diaphragmatic function before and after surgeries. Furthermore, these values can also predict diaphragmatic dysfunction and deconditioning [ 15 ]. They can be applied as a predictor of mechanical ventilation-induced diaphragm dysfunction, too [ 16 ]. The unequal distribution of age groups, the disparity of BMI among different age groups, together with the inability to perform a simultaneous assessment of pulmonary functions and diaphragmatic motion by ultrasound due to technical difficulties are the main limitations of this study. The study included only Egyptian volunteers, which may be considered another limitation, so large worldwide studies are recommended to reach worldwide normal values that can be applied to all countries. Also, further studies are needed for assessments of diaphragmatic functions in patients with chronic respiratory diseases.
Diaphragmatic excursion values presented in this study can be used as reference values to detect diaphragmatic dysfunction in clinical practice. There is a significant statistical difference between right and left hemidiaphragmatic movement during all types of breathing (quiet, deep and sniffing). Age, sex and BMI significantly affect diaphragmatic motion with variable extents during different types of breathing. The assessment of diaphragmatic motion by ultrasound could be a useful indicator for the diagnosis and follow up of respiratory diseases, and could be added to outcomes in clinical trials. Further studies to assess other factors that may affect the diaphragmatic motion including metabolic factors and other anthropometric parameters are required.

1. Download the Taber's Online app by Unbound Medicine
2. Log in using your existing username and password to start your free, 30-day trial of the app
3. After 30 days, you will automatically be upgraded to a 1-year subscription at a discounted rate of $29.95
Type your tag names separated by a space and hit enter

There's more to see -- the rest of this topic is available only to subscribers.
2. Select Try/Buy and follow instructions to begin your free 30-day trial
We're glad you have enjoyed Taber's Online! As a thank-you for using our site, here's a discounted rate for renewal or upgrade.
Mobile + Web Renewal
1 Year Subscription
Consult Taber’s anywhere you go with web access + our easy-to-use mobile app.
Nursing Central
Nursing Central combines Taber’s with a medical dictionary, disease manual, lab guide, and useful tools.
Not now - I'd like more time to decide
Want to regain access to Taber's Online?
Renew my subscription
Log in to Taber's Online
Forgot your password, forgot your username, contact support.
- unboundmedicine.com/support
- [email protected]
- 610-627-9090 (Monday - Friday, 9 AM - 5 PM EST.)
Excursion of the flexor digitorum profundus tendon: a kinematic study of the human and canine digits
Affiliation.
- 1 Orthopaedic Bioengineering Laboratory, University of California, San Diego 92093.
- PMID: 2303949
- PMCID: PMC9730741
- DOI: 10.1002/jor.1100080203
The most common problem following primary flexor tendon repair is the failure of the tendon apparatus to glide, secondary to the formation of adhesions. Early motion following tendon repair has been shown to be effective in reducing adhesions between the tendon and the surrounding sheath. Therefore, it is important to determine the amount of flexor tendon excursion along the digit during joint motion. In this study, the excursion between the flexor digitorum profundus (FDP) tendon and the sheath was examined in both human and canine digits. Based on roentgenographic measurements and joint kinematic analysis, the motion of the bones, the FDP tendon, and the sheath were measured with respect to joint rotations. It was found that the canine flexor tendon apparatus behaved similarly to that of the human for the motions studied. The amount of tendon excursion was very small in regions distal to the joint in motion (approximately 0.1 mm/10 degrees of joint rotation). There was little displacement of the sheath (0.2-0.3 mm), except at the metacarpal joint region during metacarpophalangeal (MCP) joint motion and at the proximal interphalangeal (PIP) joint region during PIP joint motion. Tendon excursion relative to the tendon sheath was the largest in zone II during PIP joint rotation (1.7 mm/10 degrees of joint rotation). These results suggest that PIP joint motion may be most effective in reducing adhesions following tendon repair in zone II.
Publication types
- Research Support, Non-U.S. Gov't
- Research Support, U.S. Gov't, P.H.S.
- Fingers / anatomy & histology
- Fingers / physiology*
- Joints / anatomy & histology
- Joints / physiology
- Metacarpophalangeal Joint / anatomy & histology
- Metacarpophalangeal Joint / physiology
- Metacarpus / anatomy & histology
- Metacarpus / physiology
- Movement / physiology
- Tendons / anatomy & histology
- Tendons / physiology*
Grants and funding
- R01 AR033097/AR/NIAMS NIH HHS/United States
- AR 33097/AR/NIAMS NIH HHS/United States
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
12 2.2.3 Types of Body Movements
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 1 ).
Human movements are complex. In order to describe movements we typically break down the movement and describe what is occurring at every joint. At each joint, we can break down the movement into three planes. Planes describe the direction of the movement. The sagittal plane lies vertically and divides the body into right and left parts. Forward and backward movements fall into this plane (flexion, extension). The frontal plane also lies vertically but divides the body into anterior and posterior parts. Lateral movements that involves the limbs moving away and towards the body fall under this plane (adduction, abduction). The transverse plane lies horizontally and divides the body into superior and inferior. Rotations and twisting motions fall under this plane (internal rotation, external rotation).
An axis is a straight line around which a limb rotates. Movement at a joint takes place in a plane about an axis. There are three axes of rotation that correspond to each of the three planes:
- Sagittal plane: medio-lateral axis
- Frontal plane: anteroposterior axis
- Transverse plane: longitudinal axis
There is a tendency when describing a movement to refer it to the particular plane that it is dominated by. For example, running is often considered to be a movement in the sagittal plane. In reality, all movements involves movements in more than one dimension.
Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 1 as you go through this section.

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 1 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 1 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 1 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 1 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 2 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 2 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 2 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 2 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 2 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 2 l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
Answers for Review Questions
Answers for Critical Thinking Questions
- Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
- To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
Biomechanics of Human Movement Copyright © August 22, 2016 by OpenStax is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.
Share This Book
- Media Library
- Encyclopedia
- Universities

Unlock with Premium
- Dynamic occlusion: lateral excursion
The dynamic occlusion is the contact that teeth make during movements of the mandible - when the jaw moves side to side, forward, backward or at an angle. In dynamic occlusion, the contacts of the teeth are not points as in static occlusion, but they are described with lines.
- Dental occlusion
- Occlusal relationship
- Temporomandibular joint (TMJ)
- Joint capsule and ligaments of TMJ
- Movements of TMJ
- Static occlusion: centric occlusion
- Occlusion concepts: centric relation
- Angle's classification
- Angle's classification: Class I
- Angle’s classification: Class II, Division 1
- Angle's classification: Class II, Division 2
- Angle's classification: Class III
- Dynamic occlusion: canine guidance
- Dynamic occlussion: protrusion
- Curve of Spee
- Curve of Wilson
- Sphere of Monson
- More from M-W
- To save this word, you'll need to log in. Log In
Definition of excursion
Did you know.
In Latin, the prefix ex- means "out of" and the verb currere means "to run." When the two are put together, they form the verb excurrere , literally "to run out" or "to extend." Excurrere gave rise not only to excursion but also to excurrent (an adjective for things having channels or currents that run outward) and excursus (meaning "an appendix or digression that contains further exposition of some point or topic"). Other words deriving from currere include corridor , curriculum , and among newer words, parkour .
Examples of excursion in a Sentence
These examples are programmatically compiled from various online sources to illustrate current usage of the word 'excursion.' Any opinions expressed in the examples do not represent those of Merriam-Webster or its editors. Send us feedback about these examples.
Word History
Latin excursion-, excursio , from excurrere
circa 1587, in the meaning defined at sense 1a
Theme music by Joshua Stamper ©2006 New Jerusalem Music/ASCAP
Get Word of the Day delivered to your inbox!
Dictionary Entries Near excursion
excursional
Cite this Entry
“Excursion.” Merriam-Webster.com Dictionary , Merriam-Webster, https://www.merriam-webster.com/dictionary/excursion. Accessed 24 Apr. 2024.
Kids Definition
Kids definition of excursion.
from Latin excursio, excursion- "a going out," from excurrere "to run out, make an excursion, extend," from ex- "out, forth" and currere "to run" — related to current
Medical Definition
Medical definition of excursion, more from merriam-webster on excursion.
Nglish: Translation of excursion for Spanish Speakers
Britannica English: Translation of excursion for Arabic Speakers
Subscribe to America's largest dictionary and get thousands more definitions and advanced search—ad free!

Can you solve 4 words at once?
Word of the day.
See Definitions and Examples »
Get Word of the Day daily email!
Popular in Grammar & Usage
More commonly misspelled words, commonly misspelled words, how to use em dashes (—), en dashes (–) , and hyphens (-), absent letters that are heard anyway, how to use accents and diacritical marks, popular in wordplay, the words of the week - apr. 19, 10 words from taylor swift songs (merriam's version), 9 superb owl words, 10 words for lesser-known games and sports, your favorite band is in the dictionary, games & quizzes.

IMAGES
VIDEO
COMMENTS
Retrusion in Anatomy. Retrusion is the opposite of protrusion. It refers to the movement of a structure in a posterior, or backward, direction. Putting your tongue back in your mouth, moving the lips back, or moving the mandible back are all examples of retrusion in anatomy. Excursion in Anatomy
Excursion. Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Excursion. Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline. Superior Rotation and Inferior Rotation
Protrusion, retrusion, and excursion are terms used in anatomy to describe body movements going anteriorly (forward), posteriorly (backward), or side-to-side...
Excursion. Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline. Superior Rotation and Inferior Rotation
Dorsiflexion and plantarflexion are terms used to describe movements at the ankle. They refer to the two surfaces of the foot; the dorsum (superior surface) and the plantar surface (the sole). Dorsiflexion refers to flexion at the ankle, so that the foot points more superiorly. Dorsiflexion of the hand is a confusing term, and so is rarely used ...
Excursion. Excursion is the side-to-side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline. Superior Rotation and Inferior Rotation
excursion. a range of movement regularly repeated in performance of a function, e.g., excursion of the jaws in mastication. adj., adj excur´sive. lateral excursion sideward movement of the mandible between the position of closure and the position in which cusps of opposing teeth are in vertical proximity.
Proper excursion and gliding of the tendon determine the efficiency of this function. Studies of the tendon excursion and gliding based on two simple mechanical concepts have resulted in several significant clinical implications. Previous article in issue; ... In normal anatomy, there is an intimate relationship between tendon excursion and ...
Excursion. Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Tendon excursion takes place as the muscle contracts and the joint rotates. The amount of tendon excursion is related to the amount of the joint rotation. A pulley-type constraint keeps the tendon path close to the bone when the tendon crosses a joint. In normal anatomy, there is an intimate relationship between tendon excursion and joint ...
medial excursion side-to-side movement that returns the mandible to the midline medial (internal) rotation movement of the arm at the shoulder joint or the thigh at the hip joint that brings the anterior surface of the limb toward the midline of the body opposition thumb movement that brings the tip of the thumb in contact with the tip of a finger
Introduction. The diaphragm is the main muscle of respiration [].Diaphragmatic excursion is 1-2 cm during tidal breathing and 7-11 cm during deep inspiration [].The assessment of diaphragmatic function is important for diagnosis and follow up of various physiologic and pathologic conditions [].Several methods exist for the evaluation of diaphragmatic function.
In mechanical terms, the wrist joint is moved by a system of effective pulleys and levers influenced by the anatomic structures present at the wrist. Assuming that the tendon excursion in a cadaver would reflect the excursion of the corresponding tendon in a live hand moving the wrist through the same arc of motion, this study measures the excursions of the wrist tendons during flexion ...
excursion. 1. Wandering from the usual course. 2. The extent of movement of a part such as the extremities or eyes. 3. In diabetes, an increase in blood glucose levels above normal or typical values, esp. after a meal. There's more to see -- the rest of this topic is available only to subscribers.
Therefore, it is important to determine the amount of flexor tendon excursion along the digit during joint motion. In this study, the excursion between the flexor digitorum profundus (FDP) tendon and the sheath was examined in both human and canine digits. Based on roentgenographic measurements and joint kinematic analysis, the motion of the ...
The eyelid margin. This diagram demonstrates the conceptual split between the anterior lamella (skin and orbicularis, right side) and posterior lamella (tarsus and conjunctiva, left side) of the eyelid. The gray line, which is the muscle of Riolan (the most superficial aspect of the orbicularis muscle), is also shown.Note that this is just anterior to the meibomian gland orifces, which come ...
Excursion. Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline. Superior Rotation and Inferior Rotation
Occlusion is an integral part of dental treatment as dentists cannot repair, move or remove teeth without affecting occlusion. 1. The masticatory system comprises the teeth, the periodontal tissues and the articulatory system. The articulatory system is in itself a triumvirate comprising the temporomandibular joint (TMJ), muscles of mastication ...
Anatomy.app 3D Anatomy. Regions ... Dynamic occlusion: lateral excursion The dynamic occlusion is the contact that teeth make during movements of the mandible - when the jaw moves side to side, forward, backward or at an angle. In dynamic occlusion, the contacts of the teeth are not points as in static occlusion, but they are described with ...
excursion: [noun] a going out or forth : expedition. a usually brief pleasure trip. a trip at special reduced rates.